Onlay bloktransplantat eller alveolær distraktionsosteogenese til vertikal knogleopbygning af processus alveolaris i den atrofiske posteriore mandibel
I nærværende oversigtsartikel præsenteres den nuværende viden om vertikal knogleopbygning af den atrofiske posteriore mandibel før implantatindsættelse ved hjælp af autolog onlay bloktransplantation og alveolær distraktionsosteogenese.
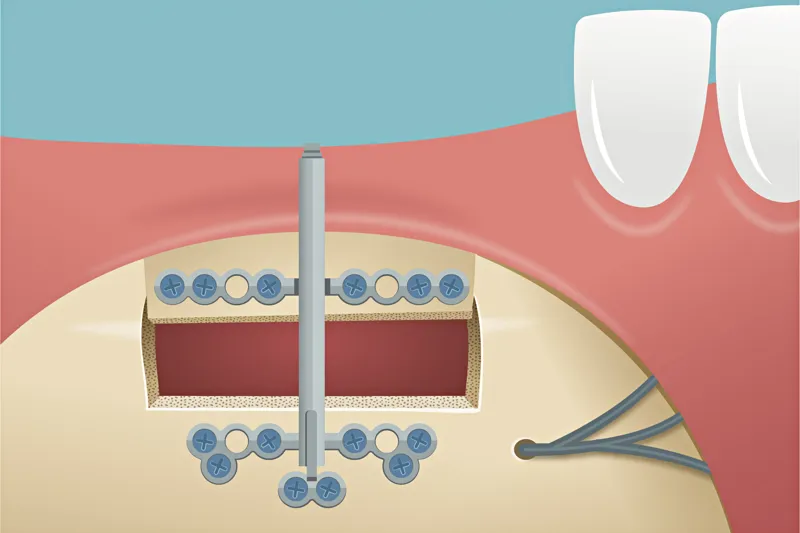
Implantatindsættelse i den atrofiske posteriore mandibel kan være vanskeligt som følge af reduceret afstand mellem toppen af processus alveolaris og den øvre begrænsning af canalis mandibulae. Indsættelse af korte implantater eller sandwichosteotomi med forsinket implantatindsættelse er de hyppigst anvendte kirurgiske teknikker til protetisk rehabilitering af klasse III- og IV-knogledefekter i mandiblen. Imidlertid kan protetisk rehabilitering med korte implantater ofte medføre en uhensigtsmæssig krone-implantat-ratio, og sandwichosteotomi kan være forbundet med utilstrækkelig øgning af processus alveolaris’ højde eller være umulig grundet insufficient knoglehøjde over canalis mandibulae. Autologt onlay bloktransplantat eller alveolær distraktionsosteogenese før implantatindsættelse har derfor været anbefalet som behandlingsalternativ for at skabe tilstrækkelig højde af processus alveolaris før implantatindsættelse og sikre en bedre udformning af den protetiske rekonstruktion. Begge behandlingsmodaliteter har vist høj implantatoverlevelse, minimalt periimplantært marginalt knoglesvind og en større øgning af processus alveolaris’ højde sammenholdt med sandwichosteotomi. Imidlertid er begge behandlingsmodaliteter særdeles kirurgisk krævende og derfor kun tilrådeligt i udvalgte patienttilfælde, hvor der er behov for betydelig øgning af processus alveolaris’ højde. Endvidere kræver alveolær distraktionsosteogenese i lighed med sandwichosteotomi tilstedeværelse af minimum 4 mm knoglehøjde over canalis mandibulae med henblik på at kunne foretage den nødvendige osteotomi. I nærværende oversigtsartikel præsenteres den nuværende viden om vertikal knogleopbygning af den atrofiske posteriore mandibel før implantatindsættelse ved hjælp af autolog onlay bloktransplantation og alveolær distraktionsosteogenese.
Klinisk relevans:
Protetisk rehabilitering af den atrofiske posteriore mandibel ved hjælp af autologt bloktransplantat eller alveolær distraktionsosteogenese før implantatindsættelse er særdeles kirurgisk krævende og forbundet med en betydelig risiko for komplikationer. Indsættelse af korte implantater eller vertikal knogleopbygning af processus alveolaris ved hjælp af sandwichosteotomi og forsinket implantatindsættelse er således det foretrukne behandlingsvalg til protetisk rehabilitering af den atrofiske posteriore mandibel.Onlay bone block graft or alveolar distraction osteogenesis for vertical bone augmentation of the atrophic posterior mandible
Implant placement in the atrophic posterior mandible can be compromised due to reduced distance between the top of the alveolar crest and the upper border of the mandibular canal. Placement of short implants or sandwich osteotomy in conjunction with delayed implant placement are the most frequently used surgical procedures for prosthetic rehabilitation of class III and IV mandibular defects. However, prosthetic rehabilitation with short implants will commonly be associated with an inappropriate crown-to-implant ratio, and the vertical augmentation of the alveolar ridge height can be inadequate following sandwich osteotomy or present with an insufficient distance to the mandibular canal to allow sandwich osteotomy. Onlay autogenous bone block graft or alveolar distraction osteogenesis prior to implant placement have therefore been recommended as a treatment option to create sufficient height of the alveolar ridge prior to implant placement and ensure a better design of the prosthetic reconstruction. Both treatment modalities have demonstrated high implant survival, minimal peri-implant marginal bone loss, and improved vertically bone gain compared with sandwich osteotomy. However, both treatment modalities are surgically demanding and thus only advisable in selected cases requiring a significant enhancement of the alveolar ridge height. In addition, the presence of a minimum of 4mm vertical bone height above the mandibular canal is a prerequisite for performing the osteotomy necessary for distraction osteogenesis. This review presents the current knowledge of vertical augmentation in the atrophic posterior mandible prior to implant placement using onlay autogenous bone block graft and alveolar distraction osteogenesis.
